The Cult of the Microbe and the Origin of ‘Preventive Medicine’ / Ethel D. Hume

From Bechamp or Pasteur?
It was at the beginning of 1873 that Pasteur was elected by a majority of one vote to a place among the Free Associates of the Academy of Medicine. His ambition had indeed spurred him to open ‘a new era in medical physiology and pathology’, but it would seem to have been unfortunate for the world that instead of putting forward the fuller teaching of Antoine Béchamp he fell back upon the cruder ideas now widely known as the ‘germ theory’ of disease. He even used his influence with the Academy of Science to anathematise the very word microzyma; so much so that M. Fremy, even though a friend of Béchamp, declared that he dared not even utter the word any more.
As a name was, however, required for airborne micro-organisms, Pasteur accepted the term microbe suggested by the surgeon Sédillot, a former Director of the Army Medical School at Strasbourg. The criticism might be made that this term is an etymological solecism; the Greeks used the word macrobiorus to denote races of long-lived people, and now a name concocted from Greek words for short-lived was conferred upon micro-organisms whose parent-stem, the microzyma, Béchamp had described as being ‘physiologically imperishable’. Man, who so seldom lasts a century, might better be called a ‘microbe’, and the microzyma a ‘macrobe’!
It was not until 1873 that Sédillot put forward his suggestion; but before this Pasteur had been busy promoting micro-organisms as the cause of varying troubles, and in 1874 he was gratified by an appreciative letter from Lister. The latter wrote that the Pasteurian germ theory of putrefaction had furnished him “with the principle upon which alone the antiseptic system can be carried out.”
However, let us turn to the verdict of time, which – according to Pasteur’s own dictum – must pronounce judgment on a scientist. Before the last Royal Commission on Vivisection, which sat from 1906 to 1908, Sir Henry Morris, President of the Royal College of Surgeons, wishing to put the best case possible for Pasteur, was forced, all the same, to acknowledge:
“In consequence of further researches and experience, some modification of the technique first introduced by Lord Lister occurred, and the evolution of the aseptic method resulted.”
Dr. Wilson points out in his Reservation Memorandum of the Royal Commission that
“…the basis of aseptic surgery, which in essence is clean surgery, was explained – as stated in the report and in reply to a question by Sir William Collins – by Semmelweiss before 1850, who attributed the blood poisoning which devastated his wards in a Viennese hospital to putrid infection, and strongly urged cleanliness as a means of preventing it.”
Dr. Wilson shows how Lord Lister brought about the application of this advice as to cleanliness considerably before his ideas were moulded by Pasteur. This latter influence, this Pasteurian theory
“…that the causa causans of septicism in wounds rested on micro-organisms in the air was an altogether mistaken theory.”
It was on this ‘mistaken theory’, this ‘principle’, provided for him by Pasteur, that Lord Lister based his use of carbolic spray, of which, before the Medical Congress in Berlin in 1891, he made this recantation:
“I feel ashamed that I should ever have recommended it for the purpose of destroying the microbes in the air.”
Thus pronounces the verdict of time against the theories of Pasteur; while as regards the teaching of Béchamp, what do we find? Dr. Wilson continues:
“The real source of all the mischief was the unclean or putrefying matter which might be conveyed by hands, dressings, or other means, to freshly made wounds.”
Such contamination is exactly explained by the microzymian doctrine, which teaches that this putrefying matter with its morbid microzymas can affect the normal conditions of the inherent microzymas of the body with which it comes into contact. Thus the verdict of time corroborates Béchamp.
Pasteur declared danger to arise from atmospheric microbes. He talked of ‘invaded patients’, and triumphantly chalked upon a blackboard the chain-like organism that he claimed to be the germ of puerperal fever.
Béchamp maintained that in free air even morbid microzymas and bacteria soon lose their morbidity, and that inherent organisms are the starting points of septic and other troubles.
What was Lord Lister’s final judgment, after having abandoned the method into which he was misled by Pasteur? Here are his own words, as quoted by Dr. George Wilson:
“The floating particles of the air may be disregarded in our surgical work, and, if so, we may dispense with antiseptic washing and irrigation, provided always that we can trust ourselves and our assistants to avoid the introduction into the wound of septic defilement from other than atmospheric sources.”
Comment is unnecessary.
But in the 1870s, the specific airborne germ theory had the charm of novelty, and its crude simplicity attracted the unscientific, although many scientists opposed it sturdily. Pasteur, however, continued upon a triumphal career of pronouncements of disease germs, and was assisted by the conclusions of Dr. Koch and other workers.
Anthrax, to which we have already alluded, offered him a convenient field for his quest of the microbe, and a little later his attention was turned to an organism first noticed by a surgeon named Moritz, and afterwards claimed by Toussaint to be responsible for chicken cholera.
This so-called microbe Pasteur cultivated assiduously, as he had already cultivated the bacillus anthracis. He also inaugurated the fashion for what may be called the study of artificial disease conditions; that is to say, instead of giving attention to Nature’s experiments in naturally diseased subjects, human and animal, the mania was aroused for inducing sickness by poisonous injections, a practice Pasteur started about this time and which his followers have so persistently copied that some have even deliberately performed iniquitous and unethical experiments upon men, women and children.
There can also be no question that since his day, bird and animal victims of every species have died and suffered in the millions all over the world in laboratories, and that had Pasteur never lived, our ‘little brothers and sisters’, to quote St. Francis of Assisi, would have been spared incalculable agonies.
His admirers will, of course, retort that his experiments were undertaken with a direct view to alleviate suffering and, in the first instance, animal sicknesses, particularly splenic fever. But it must strike anyone as a topsy-turvy method to start the cure of natural diseases by the production of artificial; and the principle of vicarious suffering can surely only hold good ethically by voluntary self-sacrifice. But we are not here so much concerning ourselves with the ethics of Pasteur’s procedure as with the practical outcome, so let us turn our attention to the unfortunate hens that were numbered among his early victims.
Pasteur tested his cultures of the so-called chicken cholera microbe on poultry, and killed birds with systematic regularity. It came about, however, that a few were accidentally inoculated with a stale culture, and these merely sickened and went on to recover. This did not, however, save them from further experiments, and these ‘used’ hens were now given a fresh dose of new culture. Again they proved resistant. This immunity was promptly ascribed to the previous dosage of stale culture. Pasteur then started to inject attenuated doses into hens, and claimed that this protected them from death when afterwards inoculated with fresh virus. His biographer asks:
“Was not this fact worthy of being placed by the side with that great fact of vaccine over which Pasteur had so often pondered and meditated?”
His meditations, however, show nothing of the caution his biographer is so anxious to ascribe to him. Vallery-Radot says:
“Original researches, new and bold ideas, appealed to Pasteur. But his cautious mind prevented his boldness from leading him into errors, surprises or hasty conclusions. ‘That is possible,’ he would say, ‘but we must look more deeply into the subject.’”
However, bold ideas had apparently only to have been made familiar over time for caution to forsake Pasteur. A true disposition of scientific doubt would have prompted him to establish the truth of the success or failure of Jennerian vaccination before accommodating accidents or theories to account for it. As a matter of fact, Koch, in 1883, would not admit that the chicken cholera prophylaxis had the value that was claimed for it; while Kitt in 1886 declared that ordinary precautions (cleanliness, isolation of infected birds, etc.), were preferable. In regard to the particular accident of the stale culture, which was made the foundation stone for the whole system of inoculation; it is evident that, like most people, Pasteur had accepted vaccination without personal investigation, and so, like many others, showed himself possessed of a simple credulity that is the antithesis to scientific cautiousness.
This criticism is the more justified because at this date in France, as in England, the subject of vaccination had become contraversial.
In 1863 Ricord, a famous French physician, was already delivering a warning against the transmission of syphilis by the practice. By 1867, the Academy had received evidence of the truth of this contention; and in 1870 Dr. A. Caron of Paris declared that he had long since refused to vaccinate at any price.
We should relate what happened when Dr. Charles Creighton was asked to write an article on vaccination for the Encyclopaedia Britannica. He complied, but being a scientist in deed as well as in name, felt it incumbent first to study the subject. As a consequence, the article had to be condemnatory, for investigation proved vaccination to be ‘a grotesque superstition’ in the opinion of the greatest of modern epidemiologists.
Pasteur, on the contrary, incautiously accepting the popular view, had a credulous belief in the success of vaccination, and made his hens’ behaviour account theoretically for a practice that he seems never to have investigated historically. It is true that he paused to notice a discrepancy between Jenner’s vaccination and the theory founded upon it. According to Pasteur, a previous injection of a stale culture safeguarded against a later injection of fresh virus; but how could two such dissimilar disease conditions as cowpox and smallpox be a protection the one from the other? His response:
“From the point of view of physiological experimentation, the identity of the variola virus with the vaccine virus has never been demonstrated.”
We are not engaged upon an anti-vaccination treatise, but as Jennerian vaccination – whether in its original form of cowpox, or its modernised guise of smallpox matter, passed (usually) through a heifer – is the foundation of Pasteurian inoculation, the two subjects are linked together, and with the demolition of the first follows logically the downfall of the second. The whole theory is rooted in a belief in the immunity conferred by a non-fatal attack of a disease. The idea arises from the habit of regarding a disease as an entity, a definite thing, instead of a disordered condition due to complex causes; the germ theory of disease, in particular, being the unconscious offspring of the ancient Eastern faith in specific demons, each possessed of his own special weapon of malignity. Thus the smallpox inoculation introduced into England from Turkey by Lady Mary Wortley Montague in the eighteenth century and its Jennerian substitute of cowpox inoculation were based on the ancient Indian rite of subjecting people to an artificially induced attack of smallpox to propitiate Sheetula-Mati, the goddess of that torment.
Believers in the doctrine of immunity may correctly retort that seeming superstitions are often founded upon the observations of experience. Be that as it may, what remains for the lover of accuracy is to examine each superstitious belief upon its own merits and test the facts of life in regard to it. The assertion that because many people have had a one and only attack of any specific complaint, an auto-protection has thus been afforded them is surely no more scientific than the old Indian belief in the assuaging of the wrath of a malignant goddess.
As Professor Alfred Russel Wallace says:
“Very few people suffer from any special accident twice – a shipwreck, or railway or coach accident, or a house fire – yet one of these accidents does not confer immunity against it happening a second time. The taking for granted that second attacks of smallpox, or of any other zymotic disease, are of that degree of rarity as to prove some immunity or protection, indicates the incapacity for dealing with what is a purely statistical question.”
Yet so imbued is medical orthodoxy with the immunity theory that we recall a doctor laying down the law on this subject even though his own daughter had recently died of a third attack of scarlet fever!
As Herbert Spencer has shown in his Principles of Psychology, there is in the genesis of nerves a great likelihood of the development of habit. All of us know how easy it is to catch colds, and that complaints such as influenza are apt to be repeated. A trifling trouble such as a cold sore may often be observed to reappear time after time in the same spot.
If we wish to theorise, it might seem probable that when the system undergoes such a thorough upheaval as that brought about by serious disorders like smallpox, the chance of recurrence is markedly less than in more trifling disturbances, such as colds and influenza. We should remember that what we call disease is often nature’s method for ridding us of poisons; and, to take a homely example from household life, while a thorough house-cleaning takes place usually once a year, the dusting of rooms is of frequent occurrence. Such a theory is, however, palpably opposed to belief in immunity through artificially induced disorders, and, moreover, plausible though it may seem, it is contradicted by statistical evidence.
The testimony of Professor Adolf Vogt, who from 1877 to 1894 was Professor of Hygiene and of Sanitary Statistics in the University of Berne, Switzerland, is quoted by Professor Alfred Russel Wallace in Chapter 18 of The Wonderful Century.
Using the statistical data available to him at the time, Vogt supplied a mathematical demonstration that a person who had undergone smallpox once was 63% more liable to suffer from it again in a subsequent epidemic than a person who had never had the disease. Vogt concluded:
“All this justifies our insisting that the theory that immunity can be confered by a previous attack of smallpox – whether the natural disease or the disease produced artificially – must be relegated to the realm of fiction.”
Certainly, if no auto-prophylaxy is induced by natural disorders, no claim can surely be made for auto-prophylaxy from artificially provoked disturbances.
In regard to vaccination against smallpox, experience can be our guide, since we have a whole century’s history to consider with regard to its efficacy. We are faced by outstanding facts, from among which we may quote an illustrative example provided by Professor Wallace in Chapter 18 of The Wonderful Century.
In it he shows how free vaccination was offered in 1840, made compulsory in 1853, and in 1867 the order was given to prosecute evaders; and so stringent was the application of the regulations that few children escaped vaccination. Thus the following table provides a striking illustration of the inefficacy of vaccination in regard to smallpox mortality:
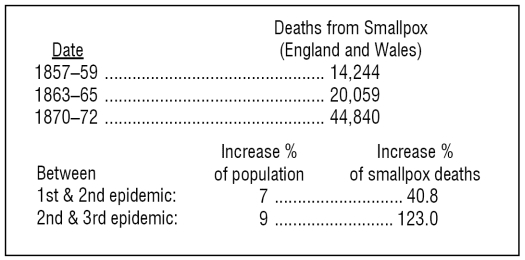
These figures show that while the population went up only 7% and 9% in the years covered, smallpox mortality increased at the rate of 40.8% and 123% – and this in face of an ever increasing number of vaccinations!
Now let us turn to some military testimony, since in all countries the armed forces are the most thoroughly vaccinated members of the community.
In January 1899, Chief Surgeon Lippencott of the U.S. Army, writing from Manila, said:
“The entire Command has been vaccinated at least four times since the appearance of the disease (smallpox).”
In the following March, he wrote again to state that all danger was over. However, in the reports of the Surgeon-General of the U.S.A. Army are to be found the following figures of smallpox cases and deaths:

During the same period, the smallpox fatality rate among the far less vaccinated general population of the United States did not exceed 3%!
To turn back to The Wonderful Century, Professor Wallace provides a comparison between the British Army and Navy and the unvaccinated inhabitants of Leicester during a period when the fighting forces on land and sea, at home and abroad, were stated to have been ‘completely revaccinated’. Leicester is taken as an example because of the unvaccinated condition of almost all its inhabitants since the smallpox outbreak of 1871–2. Before this, 95% of the children born were vaccinated, and the huge attack and death rates during the epidemic were sufficient to prove the futility of vaccination. The authorities were, therefore, led to try improved sanitation and isolation as preventives, and have been rewarded not only with comparative freedom from smallpox, but also with the best health rate of all the industrial towns of Great Britain.
Professor Wallace writes as follows:
“The average annual smallpox death rate of this town (Leicester) for the 22 years 1873–94 inclusive is thirteen per million (see 4th Report, p.440); but in order to compare with our Army and Navy we must add one-ninth for the mortality at ages 15–45 as compared with total mortality, according to the table at p.155 of the Final Report, bringing it to 14.4 per million, when the comparison will stand as follows:
Army: 37.0
Navy: 36.8
Leicester (ages 15-45): 14.4Smallpox death rate per million, 1873–94
It is thus demonstrated that all the statements by which the public has been reassured as to the almost complete immunity of the revaccinated Army and Navy are absolutely false. There is no immunity. They have no protection. When exposed to infection, they suffer not just as much as other populations, but even more. In the nineteen years 1878–1896 inclusive, unvaccinated Leicester had so few smallpox deaths that the Registrar-General represents the average by the decimal 0.01 per thousand population, equal to ten per million, while for the twelve years 1878–1889 there was less than one death per annum! Here we have real immunity, real protection; and it is obtained by attending to sanitation and isolation, coupled with the almost total neglect of vaccination. Neither the Army nor Navy can show any such results as this.”
And the lessons of the past continue up to the present in Leicester, where for the 26 years ending 1931, there have been only two deaths from smallpox.
Similarly, the experience of Germany and of Japan shows us that with much vaccination there is also much smallpox, while the Philippine Islands provide us with the most striking example on record.
Since the taking over of the islands by the USA, every attention has been paid to the perfecting of sanitation. But not content with this, their Public Health Service has undertaken the thorough and systematic vaccination of the population, adding thereto a considerable amount of serum inoculation.
For the result, let us turn to an American paper, published in Minneapolis, The Masonic Observer of the 14th January, 1922:
“The Philippines have experienced three smallpox epidemics since the United States first took over the Islands, the first in 1905–6, the second in 1907–8, and the third and worst, the recent epidemic of 1918–1919.
Before 1905 (with no systematic general vaccination) the case mortality was about 10%. In the 1905–6 epidemic, with vaccination well started, the case mortality ranged from 25% to 50% in different parts of the Islands. During the epidemic of 1918–19, with the Philippines supposedly almost universally immunised against smallpox by vaccination, the case mortality averaged over 65%.
These figures can be verified by reference to the Report of the Philippine Health Service for 1919, p.78. These figures are accompanied by the statement that “the mortality is hardly explainable”. To anyone but a Philippine Medical Health Commissioner, it is plainly the result of vaccination.
Not only has smallpox become more deadly in the Philippines, but, in addition:
‘The statistics of the Philippine Health Service show that there has been a steady increase in recent years in cases of preventable diseases, especially typhoid, malaria and tuberculosis.’”
– The 1921 Report of the Special Mission on Investigation to the Philippine Islands, of which General Leonard Wood was head
Going more into detail in an earlier issue (10th December, 1921), The Masonic Observer writes:
“The highest percentage of mortality, 65.3%, was in Manila, the most thoroughly vaccinated place in the Philippines; the lowest percentage of mortality, 11.4%, was in Mindanao, where, owing to the religious beliefs of the inhabitants, vaccination had not been practised as much as in most other parts of the islands.
To the everlasting shame of the misnamed ‘Health’ Service, vaccination has been forced on Mindanao since 1918, despite this proof that their people were safer without it, and, as a result, smallpox mortality increased to above 25% in 1920.
In view of the fact that sanitary engineers had probably done more in Manila to clean up the city and make it healthy than in any other part of the islands there is every reason to believe that excessive vaccination actually brought on the smallpox epidemic, in spite of the sanitary measures taken to promote health.”
Again, from the issue of the 17th December, 1921:
“Think of it – less than 11 million population in the Philippines and 107,981 cases of smallpox with the awful toll of 59,741 deaths in 1918 and 1919. Bear in mind that, in all human probability, the inhabitants of the Philippines are as thoroughly vaccinated and revaccinated as any people in the world.
Systematic vaccination started in the Philippines in 1905 and has continued ever since. It is certain that over ten million vaccinations for smallpox were performed in the Philippines from 1905 to 1917, and very probable that the vaccinations numbered even as many as fifteen million during that time. This can be verified by reference to reports of the Philippine Health Service.”
Turning to those reports, we find evidence that the facts must have been even worse. In letters to the Secretary of Public Instruction, Dr. V. de Jesus (the Director of Health) states that in 1918 and 1919 there were in the Philippines 112,549 cases of smallpox with 60,855 deaths. The Chief of the Division of Sanitation in the Provinces gives yet higher figures for the year 1919, increasing the total for the two years to 145,317 cases and 63,434 deaths.
So the facts pronounce firmly against Jenner and Pasteur. Yet, basing his theories upon a practice already discredited by those who had given it close and impartial scientific study, Pasteur proceeded to inaugurate a system of preventive medicine focused on what he proclaimed to be the ravages of airborne microbes. The attenuated doses which, according to his theory, were to prevent natural diseases did due honour to Edward Jenner by being called vaccines.
Pasteur’s son-in-law tells us:
“Midst his researches on a vaccine for chicken cholera, the etiology of splenic fever was unceasingly preoccupying Pasteur.”
Although a vaccine for the former complaint was the first he professed to discover, it was in regard to splenic fever that a great stir was occasioned; for Pasteur was called upon in various instances to test his method of vaccination.
We will, therefore, include in the next chapter a study of his methods against anthrax, which form the starting point of the subsequent mania for inoculation which has proved so financially profitable to the manufacturers of vaccines and sera and has so disastrously polluted the advance of science with the pecuniary considerations of commercial interests.
END